
Further Communication on “Sickle Cell Trait Misinformation and Disinformation” and Sickle Cell Terminology: Disease or Disorder?
From: An Appreciative and Concerned Reader [Email details withheld]
Sent: 12 December 2011 09:20
To: felix@konotey-ahulu.com
Subject: Sickle Cell Trait Misinformation and Disinformation
Dear Professor Felix Konotey-Ahulu,
First I would like to thank you for publishing such an authoritative article on the topic of Sickle Cell misinformation and the dangerous consequences to African people.
I would like your permission to reproduce the article on our website [details withheld]
However if I may make one suggestion and request for an editorial adjustment. It is the belief of our organisation that, at least in the UK the institutional reference of Sickle Cell Disorder as a ‘disease’ is also a contributory factor to the stereotypes and the detrimental prejudicial treatment African people receive in the medical field when the topic is being raised or researched.
As such we identify Sickle Cell (SS or SC) as a genetic blood disorder and not a ‘disease’.
Whilst Sickle Cell may be accurately classified as a genetic variation, in the case of AS and in some instances of SC there are no or very little adverse effects to qualify it as a substantive impairment of normal physiological functioning. Clearly the label ‘disease’ is redundant in this instance.
We appreciate that the definition is fluid and traditionally includes disorders but the labelling of those with Sickle Cell in this manner also adds significant and to our mind unnecessary adverse social and psychological factors.
Including unwarranted fears of transmission as if it were a virus.
Your thoughts on this matter would be greatly appreciated.
Peace
[Name & address mentioned but not published here]
Dear [Writer]
Thank you so much for writing. Your comments are important, very important, but as one who has lived with siblings who had inherited a beta globin gene variant from both our parents I cannot agree that what my parents called “this hereditary disease”, and my siblings themselves also called “this aching disease” should now be called “not a disease”.
On the contrary, in all the 3 International Achievers Conferences that I conducted (First at the Royal Society of Medicine in London 1993, Second in Accra 1995, and Third Accra 2010) the participants were glad to state that although they had/have an hereditary disease (ACHE gene from mother and ACHE gene from father, making them ACHEACHE), they had been able to achieve in life and do extraordinary things – sometimes better than their brothers and sisters who did not inherit ACHEACHE.
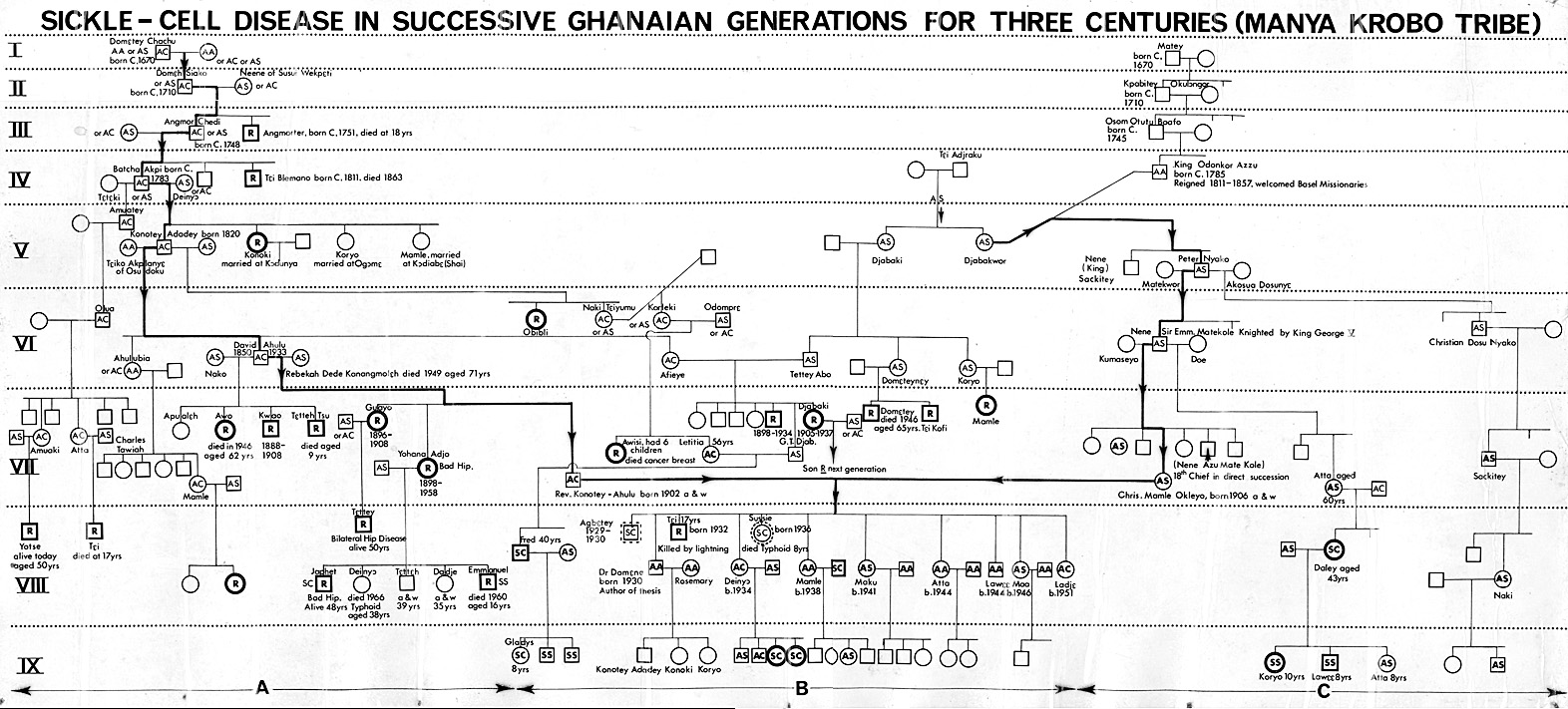
You have probably seen how I traced the sickle cell affliction or ailment (if we must avoid the word “disease”) in my own family for 9 successive generations from 1670 AD – http://www.konotey-ahulu.com/images/generation.jpg or http://www.sicklecell.md/images/generation.jpg Now, Writer, if my parents and ancestors of my Krobo Tribe in Ghana had refused to call Chwechweechwe/hemkom a disease, how would they have been able to name every single sufferer for more than 3 Centuries? Just look at the internet link yourself, and see the names of my 3 siblings with “the disease” (Generation VIII centre columns marked ‘R’ for Rheumatism inherited). The Tribal names (for example Aromolegun or Lakuregbee in Yoruba) describe the “disease” in West Africa. If some people do not want to use “disease” we can use the Yoruba “Aromolegun” but how many nurses and doctors in Europe will know what we are talking about? And if you say “Sickle Cell Blood Disorder” are many UK Doctors not calling Sickle Cell Trait a “Blood Disorder”?
{kind=link}
{kind=link}
I agree that although Diabetes is a disease, a sufferer would prefer to be said to “have Diabetes” to “suffering from Diabetes Disease”. I grant you that, so would my Patient Achievers prefer to be said to “suffer from Sickle Cell Anaemia”? Well, genetically, the term “Sickle Cell Anaemia” is reserved for “SS” where both mother and father donate the sickle cell gene “S”. The term “Sickle Cell Anaemia” cannot be used for someone who gets Haemoglobin “C” (an ACHE gene) from one parent, and sickle cell gene “S” (another ACHE gene) from the other parent, even though they too suffer severe cold season rheumatism. We call them “SC” phenotype, while Sickle Cell Anaemia persons are “SS” phenotype.
Looking after well over one thousand patients who ached in the cold rainy season in Ghana, it was clear that not all of the aching genes were “S”. Some were “C”; others were “D”, “F-hereditary”, “beta-Thalassaemia”, and so on but when inherited together with “S” from the other parent, those who suffer the aches, possess TWO aching haemoglobins, not one as in Sickle Cell Trait. Possessing one ACHE ‘S’ gene and one NORMAL ‘A’ gene does not cause the NORMACHE ‘AS’ person to have cold season rheumatism attacks called sickle cell crises.
So, Writer, as “A” is the Normal Adult Human Haemoglobin Type (never to be confused with Blood Group A), if it is inherited with “S” the person becomes “AS” (Sickle Cell Trait) which is neither a disease nor a disorder. If Normal Haemoglobin gene “A” is not present, then whatever other combination is inherited from the parents becomes “Hereditary Disease”, like ‘SS’, ‘SC’, ‘SD’, ‘Sbeta-Thalassaemia’, ‘CC’, and so on.
Each of these phenotypes has its peculiar characteristics but what is common to them is that they ALL ache in the cold rainy season. The peculiar characteristic of the “SS” is severe anaemia (inadequate blood level), this is why it, and it alone, is the phenotype called “Sickle Cell Anaemia”. A lady with “SC” phenotype cold season rheumatism who, because of heavy periods becomes severely anaemic is not called “Sickle Cell Anaemia”. She is said to have “Sickle Cell Disease ‘SC’ phenotype, with anaemia”.
The peculiar characteristic of the “SC” is not severe anaemia, but eye problems and bleeding into the eye. Sbeta-Thalassaemia persons suffer hip problems as well as cold season rheumatism. Now, in order to help my Ghanaian patients understand what I am just trying to explain to you, way back in 1973, I coined the term ACHEACHE to describe anyone who had inherited an ‘ACHE’ Haemoglobin from both parents, like three of the 11 children of my NORMACHE parents did.
Those of my patients who may not want to say things like “I have Sickle Cell Disease” do quite happily describe themselves as “I am ACHEACHE ‘SS’” or “ACHEACHE ‘SC’”. Other Achievers, some of whom became international lawyers were content to describe themselves as “I have Sickle Cell Anaemia ‘SS’” or “I suffer from Sickle Cell Disease ‘SC’”. They less prefer to be told they have a “Sickle Cell Disorder” – a term that unscrupulous Insurance companies love to extend to the Trait parents of ACHEACHE patients. No one has a just reason to look down on a person suffering from any disease, hereditary or otherwise.
If we change the terminology to “Sickle Cell Disorder”, as they do in the UK, the confusion is even greater. Many, many doctors whom I have met in the UK do a sickle cell test on someone and when the person turns out to be “AS” (Sickle Cell Trait), they then say things like “So and so has the Sickle Cell Disorder”. That kind of statement leads to the kind of misguided recommendation that “Negro travellers be tested for sickle cells for their own safety”. I hope this lengthy explanation helps a bit.
In conclusion, with “Abnormal Haemoglobins” genetically, we reserve the term “hereditary disease” for TWO ACHING HAEMOGLOBINS. The term “Sickle Cell Disease” is a Genetic Definition [Two gene variants or 2 abnormal haemoglobin genes] which can never be applied to the Trait [one gene variant]. As soon as “Disorder” comes into common use then if the blood test shows “Sickle Test Positive” the Trait (One ‘S’ gene) is considered (wrongly) as much a “disorder” as the two gene variant possessor. One sickle cell gene plus one normal ‘A’ gene does not turn the owner ‘AS’ into a sufferer. Indeed, in Africa, the child with ONE aching gene is healthier than both the one with no aching genes at all (the “AA”) and the one with two aching genes (“SS”) because the ONE ACHE gene possessor does not get cerebral malaria in childhood as do the NO ACHE possessor (“AA”) and the two-ACHE possessor “SS”). This is the phenomenon known to produce what is called Balanced Polymorphism.
Go to my FAQ (Frequently Asked Questions) on my website www.sicklecell.md or www.konotey-ahulu.com to read the reason why the “AS” phenotype is so tough. How else could we have 100 million of them in Tropical Africa? Why have they not died out if they have a “blood disorder”?
And now to your final question: Do you have permission to re-publish my article on the “Misinformation and Disinformation on the Sickle Cell Trait”?
The answer is “Yes, on condition that you also publish your query on the use of the term “Sickle Cell Disease”, and adding this response of mine above to it which forbids you from altering “Disease” to “Disorder”.
Two further points:
(a) The burden of Sickle Cell Disease (ACHEACHE) in Greece, Turkey, and other Mediterranean Countries is huge. If the White population in those countries call the hereditary condition a disease, but we Black ACHEACHE people cannot be said to have a disease, what term do we suggest for doctors, and nurses, and health workers to understand what we are talking about? If the Sickle Cell Trait is called in NHS publications “blood disorder” how do we distinguish the Sickling Positive ACHEACHE “SS” sufferer from the Sickling Positive NORMACHE “AS” non-sufferer?
We should rather aim at treating the ACHEACHE persons properly (No Morphine; No Heroin) to have them achieve their full potential in life so they can say things like; “I am the best in my Class of 50, even though I suffer from Sickle Cell Disease”.
[My own personal fact: I am the second of 11 children of my NORMACHE parents. My immediate younger brother Jerry Tei was ACHEACHE (he took Papaa’s ACHE and Mamma’s ACHE genes) yet when it came to Mathematics he was far better than I was, and I myself was extremely brilliant at the subject, scoring the second highest ‘A’ in the Achimota School Cambridge School Certificate Additional Maths Exam in those days of 120 students in the exam. Therefore far from being ashamed of being told he had Sickle Cell Disease, my brother could always say “I shall thrash you at Arithmetic, Hemkom or no Hemkom” [‘Hemkom’ meaning Sickle Cell Disease]. Why can’t British patients also take that attitude? Why can’t they take the attitude which shows that this hereditary blood disease (affliction, disorder, ailment) is no barrier to excellent academic achievement?]
(b) The more serious point is how publications in Britain label the Sickle Cell Trait a “Blood Disorder”. The question to ask is “How could a person with “blood disorder” compete with the rest of the world (as they did in the Olympic Games in Mexico City where the air was/is thin, and beat the whole world without dropping down dead?” The fact that experts in the UK can say the “Sickle Cell Trait” is a blood disorder is the reason why those of us from Africa who have seen more sickle cell traits than they have ever seen or ever can see in the UK (and lived with them in the same homes) need to continue speaking up and educating people. At least I am on record in the British Medical Journal May 27 2009 (Rapid Response) for criticising NHS material purporting to teach lay people about Sickle Cell Trait, but misleadingly referring to the NORMACHE phenotype ‘AS’ as a ‘Blood Disorder’. We can do no more than continue to point out misinformation and disinformation.
Yes, you can republish my material, but you do not have permission to editorially correct what I have said. Sure you can say “We do not agree with calling the inheritance of two abnormal haemoglobin genes ‘Sickle Cell Disease’”. But before you say that, Writer, remember that these definitions of what is ‘disease’ and what is not ‘disease’ were laid down by an International Committee.
“When in 1957 the Colonial Medical Research Committee Working Party on sickle cell trait and sickle cell anaemia recommended the use of the term ‘sickle cell disease’ the Committee meant it to denote any pathological condition that is in part attributable to sickling of the erythrocytes …including sickle cell anaemia, sickle cell Haemoglobin C disease, sickle cell Haemoglobin D disease, sickle cell beta-Thalassaemia, …” [Woodruff and Colleagues: Terminology of the hereditary haemoglobinopathies with haemoglobin variants. British Medical Journal, 1957 Volume 1, page 1235].
So, Writer, we do not unilaterally have a right to state that the term “sickle cell disease” should not be used, nor does the NHS Instruction Manual have a right to decide unilaterally to use the term “Sickle Cell Disorder” for Sickle Cell Trait. My ACHEACHE patients do not like the term ‘Disorder’. They would rather like to be said to have a hereditary disease than “blood disorder” even though our Geneva Committee used the word “disorder” to cover disease (ACHEACHE) phenotypes. They never meant it to be used for Sickle Cell Trait as the NHS Manual uses it. Well, whatever terms your ACHEACHE patients prefer to use, please use them, but point out that the cardinal confusion that arises from using “blood disorder” is that the vast majority of British Health workers will include “Sickle Cell Trait” (NORMACHE) in the “Blood Disorder” Group, which is the whole point in the first place of my “Misinformation/Disinformation” article. One wonders how many Sickle Cell Traits (NORMACHE) have also been aborted in the UK because these foetuses are officially categorized as possessing “Sickle Cell Disorder”.
But not even modern day haematologists (or patients) can change what was decided in 1957, and what we confirmed in Geneva in 1972. By “we” I mean the following: Professor Alexander Boyo, Professor Raymond Cabannes, Professor Hermann Lehmann, Dr P F Milner, Professor Bela Ringelhann, Professor D J Weatherall, Professor Italo Barrai, Professor Arno Motulsky, and Dr F I D Konotey-Ahulu [Special Expert Scientific Group on Treatment of Haemoglobinopathies and Allied Disorders, – Technical Report 1972, Volume 509, 83 pages]
My advice for all intelligent Africans is to cultivate the use of the term ACHEACHE plus the phenotype, and NORMACHE plus the phenotype. So, taking my own family, my Trait parents were NORMACHE ‘AC’ x NORMACHE ‘AS’, and their 11 children receiving variously a NORM or ACHE from them became ACHEACHE ‘SC’ (3 of us), NORMACHE ‘AS’ (2 of us), NORMACHE ‘AC’ (2 of us), NORMNORM ‘AA’ (4 of us). It is up to us to educate our doctors to many of whom all this is very strange.
When you carefully go through all my publications from 1965 to 2011 http://www.sicklecell.md/publications (or http://www.konotey-ahulu.com/publications and you decide to republish anything let me know. You may always comment on the original publications but you do not have my permission to alter what I have said.
Press on with the good work.
Have a Blessed Christmas! See my perennial Christmas Message http://bit.ly/cRcZ0s
Felix Konotey-Ahulu MD(Lond) DSc(UCC) FRCP(Lond) DTMH(L’pool)
Kwegyir Aggrey Distinguished Professor of Human Genetics, University of Cape Coast, Ghana and Consultant Physician Genetic Counsellor in Sickle Cell and Other Haemoglobinopathies, 9 Harley St., Phoenix Hospital Group, London W1G 9AL.